Understanding Chiropractic Care and Its Benefits
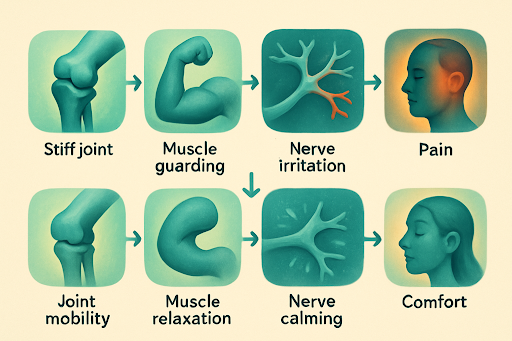
Chiropractic care is a holistic approach to health that focuses on diagnosing and treating musculoskeletal disorders, particularly those related to the spine. It aims to restore proper alignment and function, promoting overall wellness. Patients often seek chiropractic treatment for pain relief, improved mobility, and enhanced quality of life, making it an essential aspect of integrative healthcare.
The benefits of chiropractic care extend beyond just pain management. Many patients report improved posture, increased range of motion, and better sleep patterns after undergoing treatment. Additionally, chiropractic adjustments can help alleviate stress and tension, contributing to overall mental well-being. This comprehensive approach makes chiropractic care a valuable option for those looking to enhance their health holistically.
How Chiropractic Care Complements Other Treatments
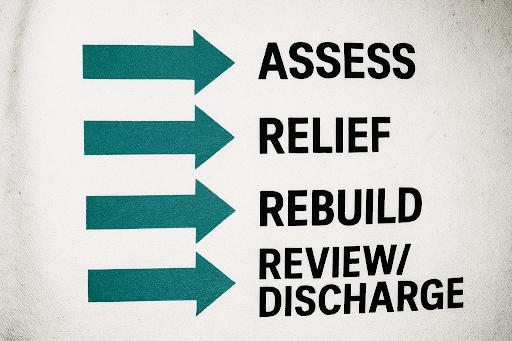
Chiropractic care is often used in conjunction with other medical treatments to provide a more comprehensive approach to health. This integrative model allows for a multi-faceted treatment plan that addresses various aspects of a patient's condition. For instance, chiropractic adjustments can enhance the effectiveness of physical therapy by improving mobility and reducing pain, allowing patients to engage more fully in their rehabilitation.
Moreover, by collaborating with other healthcare providers, chiropractors can ensure that patients receive well-rounded care tailored to their specific needs. This collaboration may include referrals to specialists, coordination of treatment plans, and shared insights on patient progress, ultimately leading to better health outcomes and patient satisfaction.
Common Misconceptions About Chiropractic Care
Despite its growing popularity, chiropractic care is often surrounded by misconceptions that can deter potential patients. One common myth is that chiropractic adjustments are painful or dangerous. In reality, most patients experience relief and comfort during and after treatments, thanks to the gentle techniques employed by trained chiropractors.
Another misconception is that chiropractic care is only effective for back pain. However, chiropractic treatment can address a wide range of conditions, including headaches, neck pain, and even digestive issues. Educating patients about the diverse applications of chiropractic care is essential to dispelling these myths and encouraging individuals to explore this beneficial treatment option.
Choosing the Right Chiropractic Treatment for Your Needs
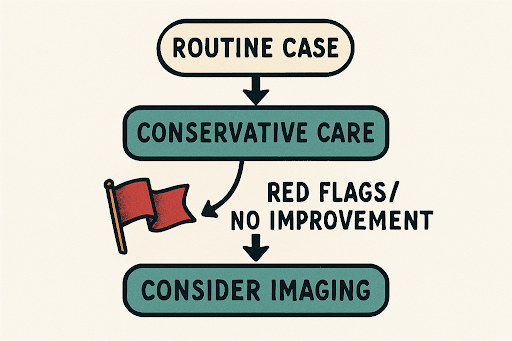
Selecting the right chiropractic treatment involves understanding your specific health concerns and goals. It's essential to communicate openly with your chiropractor about your symptoms, lifestyle, and treatment preferences. This dialogue helps the chiropractor develop a personalized treatment plan that aligns with your individual needs, ensuring you receive the most effective care possible.
Additionally, consider factors such as the chiropractor's experience, treatment techniques, and patient reviews when making your choice. A chiropractor who specializes in your specific condition or utilizes a holistic approach may offer the best outcomes. Taking the time to research and choose the right practitioner can significantly enhance your chiropractic experience and results.